|
The current COVID climate has provided me ample time and opportunity to sit back and contemplate many, many things. The first few weeks of physical distancing and working from home I found incredibly challenging. This is of no surprise to other caregivers. especially parent caregivers of children with chronic complex conditions and my bereft mother’s ‘club’. Being sequestered is a reminder of how small my world became as Sophia’s disease progressed and ultimately her last few weeks in hospice. Being a bereft parent can be an incredibly isolating space. I am heading into my third month of being in a formal role as a Patient Engagement Specialist. Having been and continue being a Patient Partner I kind of feel like a fly who is developing compound vision. Combining my decades experience as a caregiver navigating health and community systems with working on the inside has its advantages. One thing that has been popping up for me is the distinction between patient engagement and the management of. To me patient engagement or engagement in its simplest terms is a ‘relational process’. Meaning, it’s about creating, building, and entrenching relationships. It’s about interaction and connection. It’s ethical and reflexive. What I have noticed is that engagement within an institutional model or mindset tends to be more about the management of patient engagement. This includes strategic planning, coordination, organizing. The basics of management also include commanding (determining what must be done and getting people to do it) and controlling (checking progress against plans). Combining patient engagement with the management of, going back to being a fly, is like ommatidia; we have these independent units that consist of a variety of features that have the capability to distinguish innovative models and best practice. Prior to my formal role, I am not sure I understood or appreciated the management of components in patient engagement. For those who know me or are getting to know me, I consistently advocate and steward for patients and caregivers to be in positions of governance and leadership. This serves dual purpose; one, patients and caregivers will better understand what goes into the management of, and organizations or institutions will develop ethical and reflexive health care models. To me, that’s a win-win and a no-brainer. Here in British Columbia we have just hit our 100th day of COVID life. This experience across the board is highlighting the gaps and definitely emphasizing the need for change. I have had the privilege of meeting Otto Scharmer and Peter Senge and taking their U Lab program out of M.I.T. Theory U is a change management method that I, for one, am going to use more often as I straddle being an activated patient partner and a passionate patient engagement specialist. I am hopeful that as more of ‘us’ work collaboratively from within systems that those gaps will be filled and we will have better healthcare journeys that lead to better healthcare outcomes. 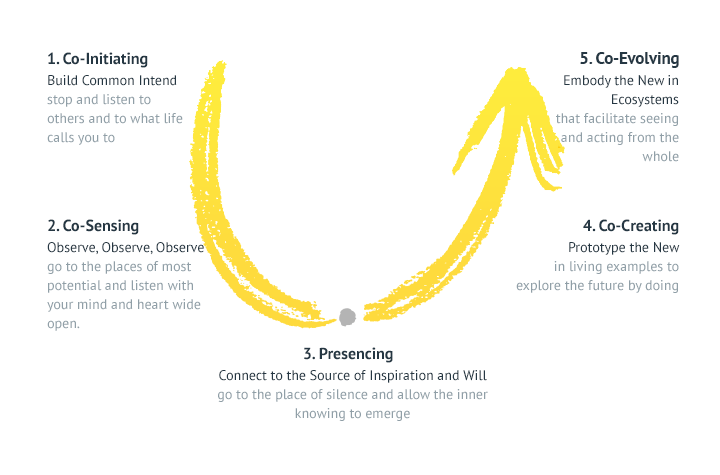
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
AuthorBeverley Pomeroy is an awarded and highly sought after Community Engagement Strategist, Speaker, Author of Living Grief; The Profound Journey of Ongoing Loss. Beverley’s community service began with a fifteen year career in private health care working for MDS Inc (LifeLabs). This community health care role developed her acumen not only for serving people in need, but also her strength in business management and organizational renewal. Archives
December 2021
Categories
|
 RSS Feed
RSS Feed