|
Our dear friend Kat Thorsen and her family and friends will be making 30 OSM (Operation Sock Monkey) sock monkeys over the holidays to donate to Canuck Place in honor of Sophia. In conjunction, San Jose State University will be doing their annual sock monkey session on January 17. 30+ folk including soldiers will be getting together to make monkeys on Zoom as part of MLK community action day. Lindsey of Operation Sock Monkey will be mentioning and honoring Sophia. Sharing Sophia's Art School site https://sophiasartschool.wordpress.com and a video of Sophia learning to draw Olaf during the summer at Stanley Park as a tribute to both Kat and Sophia and their remarkable bond through art. January 1st, 2022 marks 5 years since Sophia passed away. There have been lots of learnings over the last 5 years, in particular this last one. I have been incredibly loved and I have been incredibly crushed. I have said this before, bereft parents sit in a delicate space. Bereft parents or parents of children with chronic complex conditions are relentlessly at the intersection of trauma and grief. I have been fortunate to have won a research grant to look at that very intersection in the hopes of:
This year I have learned what, who, when and how I get pushed out of my window of tolerance. I learned that absolutely influences what I do, who I see, where I go and I have learned to allow myself permission to step away. This is hard work even when supported by an extraordinary group of professionals and may resonate for many, not just bereft parents... I cannot emphasis enough to avoid assumptions and try not to overlay others' stories into our experience. Just ask even if it may feel uncomfortable to initiate that conversation. Trees grow stronger in the wind. Evidence has shown that when we activate resiliency we create a better field of compassion. Resiliency isn't something we can get, or have, or build...it is something we can activate. And we activate resiliency by...caring connectedness, opportunities to contribute and clarity of expectations. Say that a few times. And if you take away but only one thing from my wordy post please make it CARING CONNECTEDNESS and mindfully decide what that looks like for you and the people around you. Be their sanctuary. Year 5...definitely was not my sanctuary. Living grief is still very much with me, day in day out. My grief is just as it was the moment Sophia took her last breathe. I am learning that is okay, perfectly imperfect, deep breathe in, deep breathe out. I am grateful for each of you that showed up, provided opportunities for both dialogue and silence, and learned with me along the way, This journey really is best shared. It wouldn't be a Sophia post without a quote from one of her favorite movies and characters, Olaf: "Some are worth melting for" Feel free to interpret that one on your own!
0 Comments
The current COVID climate has provided me ample time and opportunity to sit back and contemplate many, many things. The first few weeks of physical distancing and working from home I found incredibly challenging. This is of no surprise to other caregivers. especially parent caregivers of children with chronic complex conditions and my bereft mother’s ‘club’. Being sequestered is a reminder of how small my world became as Sophia’s disease progressed and ultimately her last few weeks in hospice. Being a bereft parent can be an incredibly isolating space. I am heading into my third month of being in a formal role as a Patient Engagement Specialist. Having been and continue being a Patient Partner I kind of feel like a fly who is developing compound vision. Combining my decades experience as a caregiver navigating health and community systems with working on the inside has its advantages. One thing that has been popping up for me is the distinction between patient engagement and the management of. To me patient engagement or engagement in its simplest terms is a ‘relational process’. Meaning, it’s about creating, building, and entrenching relationships. It’s about interaction and connection. It’s ethical and reflexive. What I have noticed is that engagement within an institutional model or mindset tends to be more about the management of patient engagement. This includes strategic planning, coordination, organizing. The basics of management also include commanding (determining what must be done and getting people to do it) and controlling (checking progress against plans). Combining patient engagement with the management of, going back to being a fly, is like ommatidia; we have these independent units that consist of a variety of features that have the capability to distinguish innovative models and best practice. Prior to my formal role, I am not sure I understood or appreciated the management of components in patient engagement. For those who know me or are getting to know me, I consistently advocate and steward for patients and caregivers to be in positions of governance and leadership. This serves dual purpose; one, patients and caregivers will better understand what goes into the management of, and organizations or institutions will develop ethical and reflexive health care models. To me, that’s a win-win and a no-brainer. Here in British Columbia we have just hit our 100th day of COVID life. This experience across the board is highlighting the gaps and definitely emphasizing the need for change. I have had the privilege of meeting Otto Scharmer and Peter Senge and taking their U Lab program out of M.I.T. Theory U is a change management method that I, for one, am going to use more often as I straddle being an activated patient partner and a passionate patient engagement specialist. I am hopeful that as more of ‘us’ work collaboratively from within systems that those gaps will be filled and we will have better healthcare journeys that lead to better healthcare outcomes. 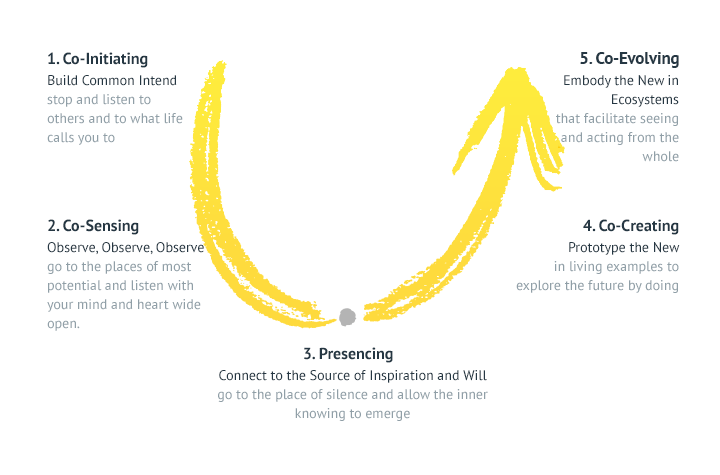 This past year there has been a lot of dialogue around patient partner compensation. It can be a thorny topic. Mostly because it goes against the grain of what we would have considered volunteering. But with the increase in patient and family engagement in research and health care there is merit in compensating patient and family partners. You can read more about this in an article written by several patient partners who have had a breadth of experience in this area; "Patient Partner Compensation in Research and Health Care: The Patient Perspective on the how and why".
The article addresses many of the challenges of patient compensation and has some great fodder for patients and health care professionals alike. Canadian Institute of Health Research has also developed Patient Compensation Guidelines that are widely used here in Canada. What I want to discuss stems from conversations I have had with patient partners who are unable to 'earn' an income due to being on disability income. Many of these patient partners have deep engagement and a true desire to help inform both research and health services based on their condition or experience. Throughout most of the patient compensation guidelines I have read, there is always the CRA (Canada Revenue Service) caveat indicating that any compensation including gift cards may be subject to taxation. For many, this is a deterrent and we are losing valuable contributions as a result. Al Etmanski is the co-founder of Planned Lifetime Advocacy Network (PLAN) and has been a tireless community organizer. Al has had incredible success in advocacy and successfully lobbied the world's first Disability Savings Plan. I decided to take a page out of Al's book and see if I could create a framework for a Canadian Patient Partner Compensation Policy. I see this as Provincially managed but Federally supported. In BC, this could be led by BC Patient and Safety Quality Council through Patient Voices Network. For anyone not familiar with Disability Assistance, it is financial and / or health support for those who have a Person With Disability (PWD) designation. PWD naturally has an annual earnings exemption allowing recipients to earn up to a pre determined amount without it impacting their monthly Disability Income. However, there is a ceiling and this is why patient partners who have a PWD designation and disability income are reticent of accepting and financial compensation despite the volume and value of their contributions. I would like to suggest we start lobbying the Federal and / or Provincial Governments to create a Federal Tax exempt income for patient partners up to a pre determined amount similar to Disability Income. The Canadian Patient Partner Compensation Policy income can surpass that pre determined ceiling but would then become taxable. Organizations 'hiring' patient partners would be responsible for any T forms similar to current practice. Now I don't profess to be a tax expert; if it isn't on Turbotax, I know nothing! But I do see more benefits than not. For one, patient partner compensation would then be a hard and steadfast line item that organizations can budget for. This also lends to ensuring funders consider patient partner compensation when determining value of grants and the costs of research; a current gap. The Canadian Patient Partner Compensation Policy (CPPCP) would also encourage standardization pay rates for patient partners. According to Indeed, the average Health Care Assistant in our Provincial Health Services Authority (PHSA) is $32.80. The CPPCP would not include or impede reimbursement of expenses like mileage, parking, travel, event registration or per diems. It may be prudent to also cap projects at 24 months in length with transition models in place should project go longer. And it would not be applicable for general volunteering like specific events, company volunteer programs, day of giving, etc. This is just a smattering of my thoughts and ideas and in no way is this a perfect framework but I strongly believe something along these lines could create equity and parity at the table and support inclusion of under represented groups and conditions. Diverse voice continues to be a gap, one we are all working hard to reduce. Curious others thoughts, ideas and perhaps, support to bring this forward to the powers that be for further discussion.  ,
When my daughter, Sophia, passed away two and a half years ago I really didn’t know when and how my life would evolve. And I certainly didn’t know how I was ever going to re-enter my professional community carrying the loss of a child. But just over a year ago I discovered a role that could provide me the opportunity to dip my toe back into health care and leverage my lived experience as a family caregiver of a child with a chronic complex condition. Here in British Columbia we are fortunate to have an organization called Patient Voices Network (PVN). PVN is a community of patients, families, caregivers working with health care partners to improve our health care system. Basically, PVN matches health care partners with patients who’s lived experience can contribute to that health care partners’ needs. That could be anything from consulting on a new process or procedure, to sitting on working groups and boards, to participating in events and sharing personal story. The opportunities are limitless and as more and more health care organizations come to understand the benefits of having patient partners, this idea is only going to grow. Through PVN I applied to posting requests that I felt resonated with me and where I felt my lived experience would contribute best. I also found opportunities on specific organization’s websites that where, again, I felt my lived experience would best serve. Very quickly I got invited to partner with a number of health care organizations; one locally (within my own community), one regionally, two provincially, and two federally. This may seem a lot from the outside, however, most of these groups meet monthly and even quarterly so the initial lift isn’t too much. Where things can get tricky is when you start participating in more specific working groups within those organizations. Very quickly your time can run away from you and you can very easily end up ‘volunteering’ chunks of your days and weeks. Note, you are volunteering…the requests come in, and you chose which, if any, working groups or projects you’d like to support on top of your otherwise monthly / quarterly commitments. This is a good sign. Health care organizations are recognizing that patients’ voices can help improve health care systems and, in the end, support better health outcomes for those in community. We have all experienced our challenges as a patient of the system so if our experience can support those working within the system, it can really be a win-win. So here I am a year later and find myself reflecting on the past twelve months as a patient partner. Naturally, some themes have emerged. For me, those themes are: Impact, Expectations and Autonomy. Impact: It is clear that having patient voices heard in a room has impact. Hearing a personal story or understanding a process or procedure through the lens of a patient changes the energy and perspective of any project. When a health care professional, a decision or policy maker can relate their work to a face, a story, it can add depth and meaning to the work they are doing. It also changes the view…for both the organization and the patient partner. I know for me, I understand far more clearly the challenges that health care organizations and employees have in their day to day than I did before being a patient partner. Being a patient partner affords me a perspective I hadn’t had before and allows me to support the group I am working with better and more effectively. In turn, the organization or group gets the benefit of understanding the impact of a procedure or process through a lived experience without risk or repercussions. I think this is one of the biggest wins for including patient voices and partnering with those who have lived experience. Ultimately, we all want the biggest impact to be better health outcomes, better patient safety, and quality improvement. And that can mean a variety of things depending on which seat you happen to be in. Expectations: This is a hard one to share as we all have our own expectations based on our desire to improve health outcomes for ourselves and our families. But expectations in relation to being a patient partner is where I feel one of the biggest challenges lie. Quite often, having a patient partner engaged is new for an organization or group. Frameworks have been developed by some who have already stepped into this realm but they are also being developed as we go along. Engaging patient partners continues to be an iterative process and I suggest that will only continue. Expectations around time, resources, reimbursement, duty, have all definitely popped up for me this past year. Depending on your skill set and depending on where an organizations’ experience lies in partnering with a patient, time and resource can be all over the place and a bit of a wild card. I had to let go of one organization because they were at the very earliest stages of including patient voices in their journey and I just didn’t have the bandwidth to be able to give them the time and thought they really needed. On another note, an organization pulled back on their commitment to a patient partner project because they just didn’t have the resources to be able to fulfill our expectations and support the projects’ needs. And that is fair… It is prudent to ask a lot of questions at the beginning of the relationship and keep those doors open to query and curiosity. Many organizations have developed patient appreciation or compensation policies as the expectations of patient partners has far outgrown traditional volunteering. You can check out the Canadian Institute for Health Research (CIHR) who has just released their recommendations. It is a great reference point. This leads to duty. As mentioned, the expectations of patient partners continues to evolve and grow and this changes our duty. This past year, I have been on health care panels, traveled to conferences, taught groups at institutions and health care faculties, participated in contributing to health care standards and quality improvements. Yea, all that in ONE year. And by choice…I wanted to test the waters, understand the dynamics of various health care initiatives, and do some discovery of what is happening in my own backyard. This volume may not be a fit for everyone so it is important to know your own expectations and capacity. I struggled to label my third and last theme. However, came up with Autonomy. And this is a controversial theme in the world of patient partners. Most of us come into a patient partner role with the greatest of intentions and the idea of servitude, as do the organizations that invite. Ideally, we have shared vision and values with the goal of improving health care for the better; impact and expectations. This is where it can get tricky and cause controversy. As patient partners we are NOT employees of any health authority, agency, organization or individual group. While we partner, we are not in any way, obligated to think, walk, talk like the group we have partnered with. Which for all intents and purposes, is why we are there. However, quite often in the last year, I have found myself in a place of what may be called ‘double consciousness’. Where in order for me to have greater impact I need to fit into the culture of the organization I am partnering with while at the same time, balancing autonomy. As patients, a lot of our experience in health care has been patriarchal, top down. That sense can be carried into our roles as patient partners where we can feel like a subordinate within the organization we partner with, or perhaps, with certain staff we have to collaborate with. Often, I have felt at the mercy of the organization or their culture. There is argument on whether or not having patient partners takes away from the patients’ autonomy and ability to have integral impact. I would have to say this is a risk and can and does happen. I am not certain of a solution other than to have independent patient partner organizations, which do exist. And quite often those organizations and members are seen as disruptors and more often than not, do not get invited to participate or collaborate within the health care system itself. As individuals, we tend to stand on our own merits and my modality has been to build relationships within organizations and health care in order to have my lived experience’s purpose reach its deepest impact. It also takes leadership, on the part of patient partners and the organizations we partner with. In fact, leadership has been one of the biggest factors in shaping my experience as a patient partner. We will leave that for another blog post! This past year has been rich with learning, full of interesting opportunities and meeting incredible people doing incredibly impacting things. I am and continue to be grateful that my lived experience has the opportunity to shift our way of thinking and improve the health care areas that I am passionate about. I think that including patient voices and having patient partners can only improve our communities for the better. And that while we still have lots to learn and there are some challenges we need to face, my own experience has been, for the most part, positive and drives me to continue this journey into the next twelve months. I appreciate all the organizations I have had the privilege of collaborating with and look forward to continuing along in my journey of healing...and finding purpose in light of tragedy. This past week has very much been ALL about patient and public engagement; where we have been, where we are and Are We There Yet? First up was listening to Carolyn Canfield's Top Ten Insights in Citizen Engagement (a Canadian perspective) during the McMaster Health Forum webinar. For those of you who don't know Carolyn, she is a pioneer in citizen engagement and patient safety, taking her tragic experience of losing her husband 8 days after surgery and redirecting that experience into deep impact around quality and safety of care in Canadian health care. Second, was watching Julia Ableson's presentation on Patient and Pubic Engagement; Are We There Yet? Dr. Ableson is the lead for the Public and Patient Engagement Research - Practice Collaborative also through McMaster. Third, was sitting in a board room with a fellow patient partner and one of our PhD researcher colleagues discussing supporting and building capacity in patient partners and researchers around patient orientated research. Now I am not terribly familiar with Dr. Ableson's work, however, a few things she shared resonated. And when I went to my meeting one thing popped up in regards to patient engagement and the IAP2 (International Association of Public Participation) spectrum of engagement that has been adopted by many in the world of patient orientated research and patient engagement. 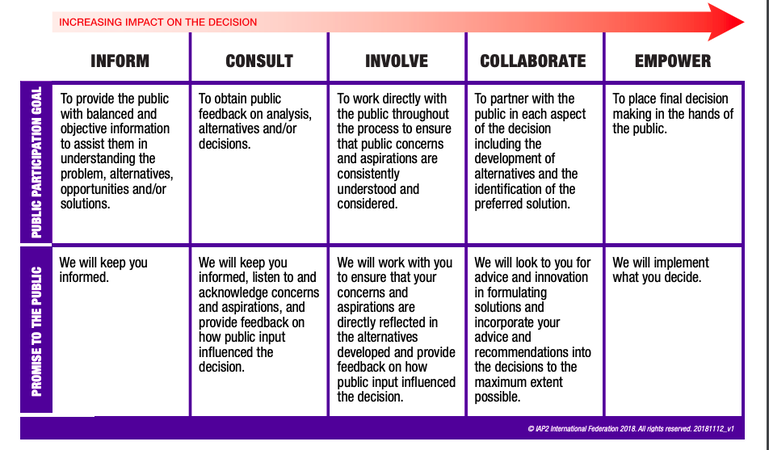 Julia actually used an older version of patient and public engagement and I didn't get a chance to ask her to share why. However, it became a focal point of my discussion later that day with my colleagues. 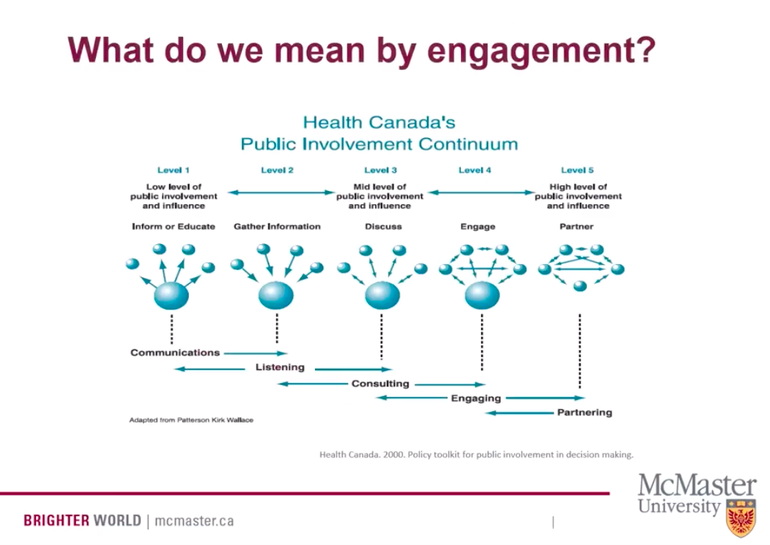 One of the comments my PhD researcher had was that we should focus on Involve, Collaborate or Discuss, Engage. His reasoning was that there is no way we will EVER get PhD researchers to 'give up control' in order for us to reach Level 5, or Empowerment in the work of patient engagement. It took me a few minutes to wrap my head around that and then I remembered Dr. Ableson's image of the public involvement continuum. And I began to reflect on my own lived experience as a caregiver navigating the health care system for two decades. My experience, despite the gut wrenching loss of my daughter in the end, has been, for the most part, a good experience with little conflict or confrontation with the plethora of health care providers we encountered.
Sensing my colleagues resolve that empowerment is a 'nice to' but 'never will be' made me feel a bit deflated. But then I shared Dr. Ableson's version of public involvement and said, look at the image used of that far right level. All the balls are the same size. I challenged the notion of power and that IF power is the hurdle to empowerment then we need to redefine what empowerment means in the IAP2 model. What I think we need to start doing and articulating is that empowerment isn't about one stakeholder having MORE power over another; ie, patient over researcher, perhaps researcher over patient. Empowerment, in its truest sense, is ALL stakeholders having equity at the table, no one group has more power. And that true empowerment in patient and public engagement is about how all of us engage and interact together for the greater good; be it research, bettering health outcomes, designing health systems, or even at the basic level...alleviating pain and symptoms of a patient or loved one. Had I not had a true partnership with my daughter, Sophia's, health care practitioners and community support workers, I am not sure her journey would have been as 'good' as it was. And ultimately, she may have died experiencing a lot more pain and discomfort than she did. My challenge to both patient partners and those in health care (researchers, health care leaders, patient engagement specialists) is that Level 5 or Empowerment IS possible...if we all come to the table with equity. And what we come to the table with, is less about power and more about forging partnerships. Interestingly enough, Carolyn Canfield's presentation was symbiotic to Julia Ableson's despite both these presenters looking at patient and public engagement from two very different lens. Which kind of makes the point... As I embark on this new iteration of my life, professionally and personally, I am committed to working towards that Level 5 of Empowerment in order to impact change. I desire to build partnerships and am keen to learn and share. I am grateful that my PhD research colleague, despite our different lens, also became excited at this redefinition of Empowerment in the work we are just beginning. And I imagine we are going to do wonderful things together...that will have lasting, meaningful impact. Last week I had the opportunity to attend BC Patient Safety and Quality Council’s Quality Forum in Vancouver as a patient partner. This was my first year attending and considering the forum was sold out in a mere three weeks, I was grateful. The Quality Forum is an annual conference, in its 7th year, featuring deep-dive sessions, presentations, and interactive workshops on a variety of topics related to improving quality across the continuum of care. In partnership with the Academic Health Sciences Network, I was invited to participate on one of the Pre-Forum panels discussing Learning Health Systems and the Critical Role of Engaging Patients with fellow patient partner, Chad Dickie and Ryan Sidorchuk, an engagement leader for BCPSQC. Stirling Bryan, Scientific Director for BC SUPPORT Unit, moderated. I was incredibly nervous participating in such an environment; being surrounded by influential health care leaders, academics upon academics, and clinical practitioners who share the front line journey alongside patients and their families. The event had over 900 attendees with patient partners making up approximately 2.5% of that. This year’s tagline was Activate, Integrate, Celebrate. It has taken me a solid week to really be able to think through and discern what themes, if any, I took away from the three day event. I can say with certainty that patient centered care was an influential theme throughout the event as was better health outcomes. Speaker Sir Chris Ham’s most positive take away from Quality Forum 2019 was patient inclusion…how great! That led me to think about my own experience in the health care system with my daughter, Sophia, and like a lot of caregivers and patients alike, we hope sharing our lived experience will impact health care delivery in positive ways. And as one prolific patient partner, Paul Caune, has coined…Hope is NOT a plan. However, I believe hope can evolve into purpose which can and does spur change. If we are to focus on patient partners in order to effect better health outcomes I think there are three distinct aspects of that; patient engagement, patient experience and patient equity. These terms mean different things to different people in different roles. However, for the sake of this blog, I am using the definition of patient engagement as set out by Fraser Health’s Awesome Handbook: ‘The term “patient engagement” is used in this handbook to describe patients participating in systems level planning. It is not used in the sense of patients being engaged in making decisions around their own individual care. “Patient” refers to a person who is currently a patient, has been a patient in the past, or is a potential future patient of health services, while “engagement” includes Ableson, et al.’s three criteria: 1) information about the issue is provided to the participants, 2) participants have the opportunity to discuss the issue amongst themselves and potentially with the decision maker, and 3) there is an explicit process for collecting the input from the participants.’ To reiterate, patient engagement is NOT ‘used in the sense of patients being engaged in making decisions around their own individual care.’ A common misunderstanding. Let me add I am also including patient families’ and informal caregivers in this conversation. Patient experience is the sum of ALL interactions that influence a patients perception across the continuum of care. So in my experience with Sophia this could entail appointments and procedures at our local Children’s Hospital. It could be our experience with Nursing Support Services, the Ministry’s At Home Program or even our interactions with our local pharmacists. Now here is where it may get prickly; patient equity. Not to be confused with health equity which amounts to offering all individuals the same chance to be healthy (that’s a whole other conversation!). If you were to search patient equity what comes up is patient capital. Patient capital is a term used in financial investment circles where an investor is willing to make a financial investment in a business with no expectation of turning a quick profit. Instead, the investor is willing to forgo an immediate return in anticipation of more substantial returns down the road. I am suggesting that the third leg in the better health outcome stool is this piece around patient equity or capital. Where we blend social and financial returns. What was evident at the Quality Forum is that there is a genuine desire to shift our health care system and delivery models to impact outcomes for ALL stakeholders. In putting a twist on traditional patient capital it is characterized by:
Speaker Rhona Flin discusses this ‘hurry up syndrome’ at a surgical level and how collective mindfulness and knowing when to slow down is as important if not more important than knowing when to speed up in practice.
After experiencing the rich content of Quality Forum 2019 and mixing that with my own lived experience as a patient partner, I am suggesting we need patient engagement, patient experience and patient equity in order to effect better health outcomes. Recognizing that patient equity or patient capital really is just my own minds way of trying to explain this piece around blending social and financial outcomes in the current system we have. How many times has a patient or family caregiver heard 'we don't have the resources for that' or 'you only have X amount of hours in nursing support', or 'X amount is covered, this amount is not'. It HAS to be a part of the conversation. In giving the final word to my daughter, Sophia, who died two years ago at the age of 16 to a complex disease process, “Take it Outside” (when referring to medical conversations in her room at the hospice), I think conferences like Quality Forum 2019 get us outside of our current thinking and open up our minds to alternative ways of ‘doing’. I am hopeful, I am full of purpose...that we can effect change together. B-HOPE: Better Health Outcomes through Patient Engagement, Patient Experience and Patient Equity   Ever since my daughter, Sophia, passed away I have struggled with…what next? I have spent 16 years as her primary care giver while juggling a variety of professional careers. I now feel at a loss of how and where I go from here.
This past year I did begin to explore where my lived experience as a caregiver may complement the world of healthcare. I became a patient partner for a variety of organizations; some federal, some provincial and some local. I have the privilege of contributing to global standards in patient engagement, of working across health authorities to lead patient priorities and to teach patient oriented programs within medical organizations. The vast majority of these opportunities are volunteer. When I began volunteering decades ago, it was mostly sitting on Family Advisory Councils, Boards or showing up at an event to share our story , or help ‘day of’. The total hours per month were maybe 3-4 max. Over the last few years, patient partners are being asked to contribute in ways that are far more complex requiring more time and acumen. And this needs to continue. I think we all agree that collaborating and co-creating in health care allows for better health outcomes. Insert your own research links here… Some organizations do have robust patient appreciation models and honorariums, and I am always reimbursed for my own incurred expenses. Yet, I mostly volunteer because I am passionate about contributing to meaningful change in our health care systems. So this leads me to patients and families as knowledge brokers. Anyone who has been or is a patient or family caregiver knows we spend an inordinate amount of time in dialogue with health care professionals, medical practitioners and community support workers in order to express our values and priorities along the way to get the best care possible. If you are someone with a rare or complex disease, quite often you are the best if not only person who can explain your disease and its impact. Knowledge Translation or KT, is a broad term for activities involved in moving research into the hands of the people and organizations who can put it to practical use. Knowledge Mobilization (KMb) refers to moving that knowledge into active use. KMb is all about making connections and is a proactive process that involves efforts to build relationships between producers and users. A Knowledge Broker is an intermediary and short of echoing Wikipedia’s definition, a knowledge broker’s key feature is to facilitate knowledge exchange or sharing between various stakeholders. Speaking from my own lived experience, I became a knowledge broker in the health and well-being of my daughter. At any given time, we were being seen and followed by no less than half a dozen if not more medical departments (neurology, endocrine, gastro-intestinal, orthopedics, renal, et al.). The list can go on and on. Toss in community support like nursing support services, physio therapy, infant development, speech therapy just to add fodder to the mix. I had to become an expert knowledge broker to ensure my daughter received the best care, at the best time and in the best way. As much as I struggle with the last few months and weeks of Sophia’s life, I do feel Sophia received the best care, at the best time and in the best way. The relationships and connections we had developed over the years saved Sophia from suffering as much as we could. Patients and family caregivers ARE knowledge brokers. It’s neither fit nor fad. We have had to learn on the fly with little information or tools along the way. Evolve us into patient partners and that brokerage becomes wider supporting researchers and leaders in health care in developing and disseminating valuable research to have more effective health outcomes. And now here is my challenge…it has come to my attention that I may be over qualified as a volunteer, yet, I am seemingly under educated to do this work professionally (no Masters in Health Sciences). While some may argue that tacit knowledge is difficult to transfer, I would argue that as a patient / family caregiver, it is quite the opposite and that partnering it with explicit knowledge is a powerful combination that can and does serve any organization willing to open their doors to the opportunity. I have a unique skill set that combines this lived experience, tacit knowledge, along with explicit knowledge that I have gained both in my professional health care career and through the various patient partner roles I have undertaken the past few years. Short of tossing my resume up on here…I am looking for an organization that may be open to creating an employment opportunity for this enthusiastic, articulate, proactive patient partner who has the capacity to contribute a strong skill set to advance health outcomes and health systems and to improve patient experiences. You can find me @beverleypomeroy (twitter and IG) or email bevcpomeroy@gmail.com  Hello and welcome to the Living Grief Podcast. Here we will discuss live, love, loss and how best to navigate this new world of living grief. Each episode will have a discussion with expert guests on grief, bereavement, living life, loss, and love. Thank you for listening to this inaugural episode. Bev
 No one tells you that there is a bottom to grief. But coming up to two years of losing Sophia, I feel like I’ve hit bottom…rock solid hard cold bottom. I sit here most days in tears. On the days I don’t, it’s because I AM in tears. On the rare occasion I can pull myself out of the dark it’s usually because someone else has dragged me out or I feel purpose in the work that I am doing that day. Living in the moment means living in the minute. The minutiae has become the strings that are holding me up, barely. When you research grief a lot of antiquated thoughts and theories are still touted as best practice and many professionals still follow those principles. But dig deep enough and you can find some sweet spots in the literature and profession. In my search for solace, I found an article in the American Psychological Associate, A New Approach to Complicated Grief written by Karen Kersting. Its dated, 2004, but much of it resonates as it speaks to new understanding of the biopsychological of the death of a loved one. A few things stood out for me. For one, in the past, the mental health community used to label bereft individuals like myself as having a ‘disorder’. Basically, if you didn’t grief in the ‘normal’ way you were labeled as ‘disordered’. With enlightened understanding and meaning around ‘complicated grief’ there are new recommendations in the way severe grief is diagnosed and being treated. I recently watched the Netflix series The Kominsky Method. Alan Arkin’s character loses his wife and ends up ‘seeing’ and talking to her on a regular basis as he navigates his new world. In Kersting’s article she shares Robert Neimeyer, PhD from the University of Memphis, research that the widely held assumption that grieving requires "letting go" is being questioned... Instead of gaining closure or trying to say goodbye, the goal of grief counselling should be to foster a constructive continuing bond with a deceased person, he says. This can be accomplished through remembering the good times, setting up an internal dialogue with a lost loved one, continuing to think of that person on a regular basis and imagining the person's reactions to current life events and problems, he says. Knowing that I have the factors for complicated grief, such as changed relationships with family and friends, feelings of meaninglessness and ruptured beliefs that have spurred health-threatening grief I figure I may just start talking to Sophia on a regular basis. What do you think? Grief is hard, so very very hard. I don’t have the answers and I am not sure anyone else does or will. But knowing it’s not about letting go is important. I need to talk to Sophia, to remember moments of joy and I am hoping that will help me lift up from bottom. If you want to help; I need work that gives me purpose. No, really I do! I need a job! I need to be gently coerced out of my cocoon. And I need to be supported in fostering a continuing bond with my beautiful, very much, missed daughter, Sophia. So if you run into me, just give me a hug, a purposeful job or a memory of Sophia that brings you joy. And, hopefully, I can slowly come up from the bottom... To listen to this blog as a Podcast, Click below  We have to feel them… It was a ridiculous time in the morning, 1:25am, and I was sitting wide awake unable to sleep. All night I had had a weird feeling in my stomach but was unable to recognize exactly what it was. I was in the ‘city’ for work and not being able to sleep in my hotel room, I got swept away watching One Mississippi on Prime Video (thanks to Amazon and Tig Notaro). I started watching the show about a month ago and the depth of vulnerability each character is able to evoke through the camera is extraordinary. I was hooked. However, on this night, there was a particular scene that clearly struck a chord with me… In a pivotal scene, Sheryl Lee Ralph’s character, Felicia, says “You cannot pretend these things have not happened. We have to feel them FULLY in order to feel anything else…” It was in that moment that I realized this particular night was the very first night I had spent alone, physically alone, since my daughter, Sophia, passed away exactly 18 months ago. Ever since the night of January 1st, 2017, I have not been alone in my own space, away from the sanctuary of my home, from the people I love, not even once. And I feel… Conveniently, I have been trying so hard not feel these past eighteen months. Countless times, I have been told ‘oh, you’re overreacting’, or ‘it’s time to move on’, or ‘you’re too emotional’. Toss in society’s innate inability to have difficult conversations or be comfortable in someone’s grief and you’ve got the perfect recipe for thinking you can’t or shouldn’t feel. Most days I find I am dismissed, invisible, abandoned even, by the people in my life I thought would show up. I have been medicated, have gone to therapy. I even tried smoking pot to ‘feel’ less; grasping for a moment of euphoric ignorance to drown my sorrow. While medication may necessary and therapy incredibly helpful… “You cannot pretend these things have not happened. We have to feel them FULLY in order to feel anything else…” I picked up my phone and began to scroll through videos I have of Sophia and I sat there that night, alone, and I gave myself permission to feel; raw, emotional, deep longing for my daughter. I realize that part of coping is feeling; and in order for me to be present in my life today, I cannot pretend Sophia didn’t die. In order for me to feel deep love, laughter or seek joy, I also need to feel my grief and sorrow FULLY in order to feel anything else. And if you’re uncomfortable with that then fuck off. Some of you already have. But for those of you who have been steadfast, tender, true…I am grateful. I long to feel ‘ok’ and maybe I won’t ever get there. But I certainly won’t stop feeling FULLY in order to appease the masses , and I certainly WILL feel fully to live my grief among the safety and sanctuary of not only those around me, but with those who aren’t.  |
AuthorBeverley Pomeroy is an awarded and highly sought after Community Engagement Strategist, Speaker, Author of Living Grief; The Profound Journey of Ongoing Loss. Beverley’s community service began with a fifteen year career in private health care working for MDS Inc (LifeLabs). This community health care role developed her acumen not only for serving people in need, but also her strength in business management and organizational renewal. Archives
December 2021
Categories
|
||
 RSS Feed
RSS Feed